
HELIOS-B Clinical Trial
HELIOS-B was a landmark clinical trial establishing the efficacy and safety of AMVUTTRA® in ATTR-CM1
A global, randomized, double-blind, placebo-controlled, Phase 3 study1-3

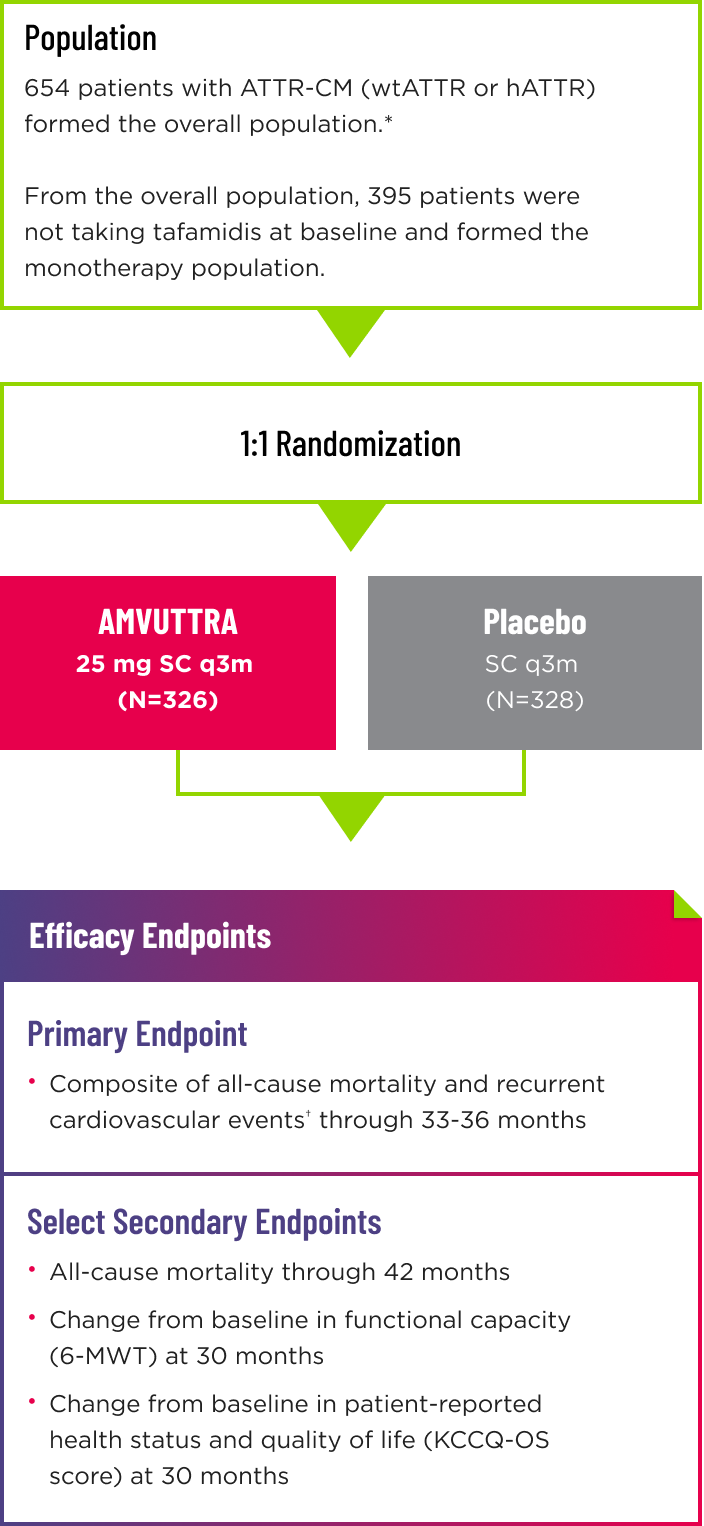
- Following the double-blind (DB) period of up to 36 months, patients on placebo were eligible to transition to AMVUTTRA in the open-label extension, which lasted up to 24 months2
- Randomization was stratified according to tafamidis use at baseline (with vs without), ATTR disease type (hereditary vs wild-type), and NYHA class and age at baseline (NYHA class I or II and age <75 years vs all others)1
*The overall population included patient cohorts with and without tafamidis use at baseline.1
†Cardiovascular events are defined as hospitalizations for cardiovascular causes or urgent visits for heart failure.1
6-MWT=6-minute walk test; ATTR=transthyretin-mediated amyloidosis; ATTR-CM=cardiomyopathy of transthyretin-mediated amyloidosis; hATTR=hereditary ATTR; mg=milligram; KCCQ‑OS=Kansas City Cardiomyopathy Questionnaire-Overall Summary; NT-proBNP=N-terminal prohormone of brain‑type natriuretic peptide; NYHA=New York Heart Association; q3m=every 3 months; SC=subcutaneous; wtATTR=wild-type ATTR.
One of the largest studies with a contemporary population of patients with ATTR-CM2,4,5*
HELIOS-B enrolled a population representative of present-day patients with ATTR-CM, characterized by2,3:
- Earlier diagnoses
- Less severe disease
- Increased heart-failure management
~80% were on diuretics at baseline
~30% started SGLT2 inhibitors during the double-blind period
- Concomitant ATTR-CM medication
~40% were on tafamidis at baseline
AMVUTTRA achieved statistically significant results across all study endpoints despite increased disease management of patients with ATTR-CM.1‑3
*Compared to other interventional pivotal studies for ATTR-CM.2,4,5
- Use of background HF medications and concomitant ATTR-CM therapy was similar across the AMVUTTRA and placebo study arms2
- SGLT2 inhibitors were added to HF guidelines in 2022, reinforcing their role as a standard of care in treatment of patients with HF6
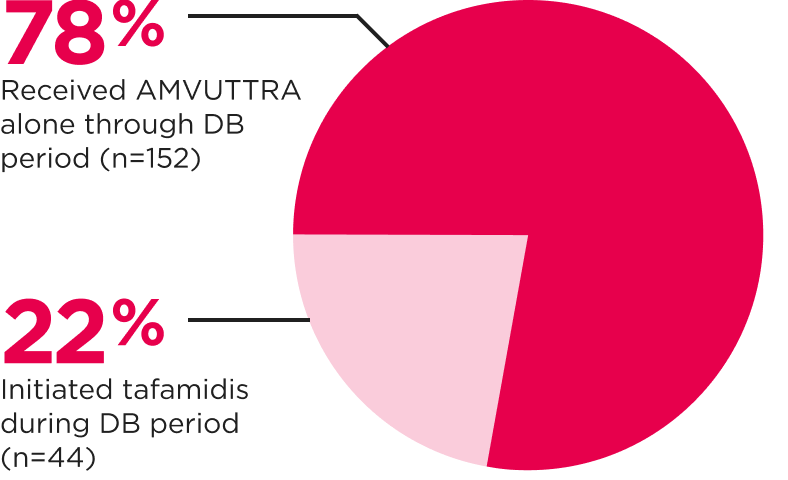
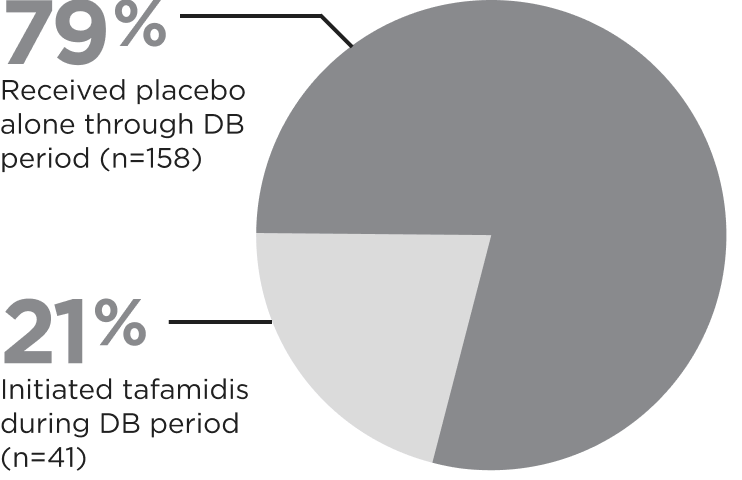
The monotherapy population comprised ~60% of patients in HELIOS-B1,2
The monotherapy population only included those not receiving tafamidis at baseline. Patients in the monotherapy population were permitted to initiate tafamidis during the DB period. The median time to initiation of tafamidis was ~18 months across both arms.
AMVUTTRA Monotherapy (n=196)3

Placebo Monotherapy (n=199)3

The monotherapy population may be representative of patients receiving first-line therapy
The study population was typical of present-day patients with ATTR-CM2
Patient Characteristics at Baseline




HF=heart failure; IQR=interquartile range; NT-proBNP=N-terminal prohormone of brain-type natriuretic peptide; SD=standard deviation; SLGT2=sodium-glucose cotransporter-2.
Patients treated with AMVUTTRA had higher NT‑proBNP and troponin I levels at baseline compared with placebo.2,3